56-year-old patient with generalised weakness, fever, shortness of breath and cough
August 31st, 2021
CHENNAMADHAVUNI DIVYA, 9th semester
Roll number-21
This is an online E logbook to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from an available global online community of experts to solve those patients clinical problems with collective current best evidence-based inputs. This e-log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment box are welcome.
I’ve been given this case to solve in an attempt to understand the topic of “patient
clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan.
Following is the view of my case:
Date of admission:-28-8-2021
Chief complaints :
A 56-year-old male patient has come to the opd with the chief complaints of, - Fever since 10 days.
- Shortness of breath since 5 days.
- Cough since 10 days.
- Generalized weakness since 15 days.
- Fever since 10 days.
- Shortness of breath since 5 days.
- Cough since 10 days.
- Generalized weakness since 15 days.
History of present illness :
The patient was apparently asymptomatic 15 days back and then he developed,Generalized weakness, which was insidious in onset and gradually progressing.Fever which was insidious in onset, high grade, intermittent in nature and associated with chills, rigours,cold,headache,loss of smell and taste sensations.
He developed shortness of breath which was in stage 2 since 15 days and has progressed to stage 4 since 5 days(MMRC classification) ,which was insidious in onset and gradually progressing ,increased on excertion and decreased on rest (supine position).
He has had productive cough which is mucoid in consistency, small in quantity,non-foulsmelling and non-blood stained, associated with pain all over the chest.
He has had joint pains for a year,Joint pains:Onset – insidiousDuration -1 yearGradually progressing, started in the knees and passed on to shoulders, lower back, arms, legs and mildly to his wrists.Not associated with swelling, tenderness.Pains are present throughout the day for a year.Type- draggingAggravating factors -work Relieving factors -not relieved on medications.
Not associated with pedal oedema, facial puffiness, palpitations, decreased urine output etc.
History of past illness :
Not a known case of Diabetes, hypertension asthma, tuberculosis, epilepsy, CVA etcSurgical history - underwent surgery for renal caliculi 10 years back.No known allergic history
Personal history :
Diet - mixedAppetite - decreasedsleep - adequateBowel and Bladder movements - regularAddictions - beedi since 30 years, 1 pack per day. Alcoholic for 10 years, 90 ml per day.
Drug history :
Family history :
No significant family history
General examination :
Patient is conscious ,coherent ,cooperative and was well oriented to time ,place and personat the time of examination.He is examined in a well lit room, with consent takenHe is moderately built and well nourishedPallor - absentIcterus - absentCyanosis - absent Clubbing - absentlymphadenopathy - absentEdema - absent
Vitals : on the day of admission (28/8/2021)
Temperature -102 degrees FPulse rate - 96 bpmRespiratory rate - 20 cpmBlood pressure - 90/50 mmHg
Day 2 -29/8/2021 :
Temperature-98.6 degree FPulse rate - 92 bpmRespiratory rate - 22 cpmBlood pressure - 130/80 mm HgSpO2- 96%GRBS - 132 mg/dl (8:00am) ,189 mg/dl (12:00 pm)
Day 3 -30/8/2021
Temperature - 98 degrees FPulse rate - 80 bpmBlood pressure - 130/70 mmHgSpO2 -98% on room air (8:00am)GRBS - 132 mg/dl (8:00am) ,120 mg/dl (8:00 pm)
Day 4 - 31/8/2021
Temperature - 98 degree FPulse rate -80 bpm (8:00am)Blood pressure -120/70 mmHgSpO2 - 96% on room air (8:00am) GRBS - 132 mg/dl (8:00am) ,138 mg/dl (2:00 pm)
Day 5 - 1/9/2021
Day 6 - 2/9/2021
Systemic examination :
CVS : S1 and S2 heart sounds heard NO murmurs and thrillsRESPIRATORY SYSTEM : Bilateral air entry present position of trachea - centrall Wheeze on inspiration was appreciatedin all the areas.Bilateral Fine crepitations where heard.
CNS : intactABDOMEN : shape of abdomen -obese Soft and non-tender No palpable masses Bowel sounds heard NO organomegaly


Investigations :
RFT : 28/8/21 (on the day of examination)
Urea - 37 mg/dlCreatinine -1.3 mg/dlSodium - 142 mEq/LPotassium -3.1 mEq/LChloride -104 mEq/L
ABG : 28/8/21 (on the day of examination)
PH - 7.5PCo2 - 22.6Po2 - 51So2 - 85HCo3 - 15.7
Random blood sugar : 28/8/21 (on the day of examination) - 123 mg/dl
RT-PCR : 28/8/21 ( on the day of admission)


Chest x-ray: 28/8/21 (on the day of admission)

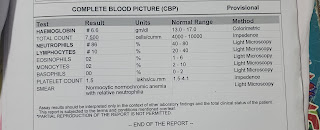
Hemogram: 28/8/21 ( on the day of admission)


Complete urine examination (CUE) : 28/8/21 (on the day of admission)

HBsAG- Rapid : 28/8/21 (on the day of admission)

HIV 1/2- Rapid : 28/8/21 (on the day of admission)

Anti HCV Antibodies : 28/8/21 (on the day of admission)

Blood grouping : 28/8/21 (on the day of admission)

29/8/21 (on day 2 of admission)

Ultrasound report : 29/8/21 (on day 2 of admission)

Review Ultrasound On 30/8/21 : diffuse abdominal tenderness.

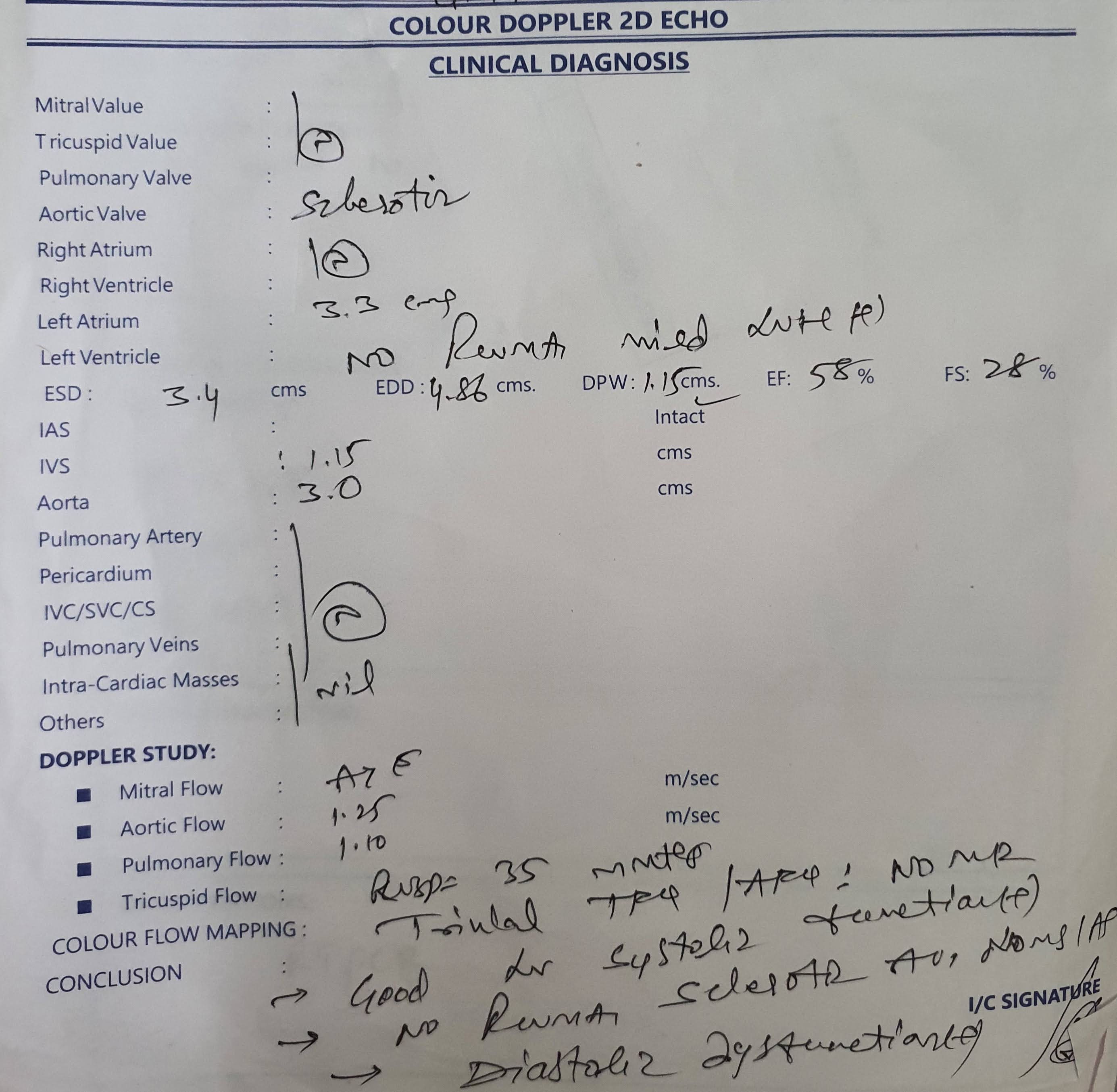
Colour doppler 2D Echo : 30/8/21 (on day 3 of admission)
ECG: 28/8/21 ( on the day of admission)



Fever charting :

Bacterial culture and sensitivity reports : 31/8/21 (on day 4 of admission)


Spirometry : 1/9/21 (on day 5 of admission)


Comments
Post a Comment